Does the Condition Affect Depth Perception or Coordination? Vision vs. Neurological Disorders Compared 2025
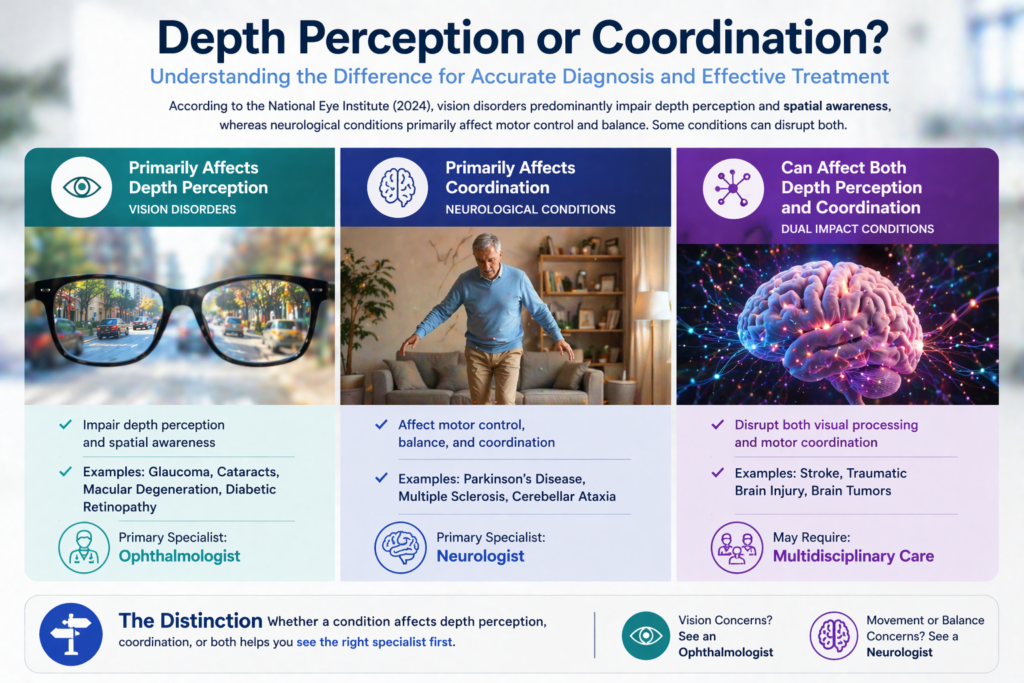
Understanding whether a medical condition primarily affects depth perception or coordination is essential for accurate diagnosis and effective treatment. According to the National Eye Institute (2024), vision disorders predominantly impair depth perception and spatial awareness, whereas neurological conditions like Parkinson’s disease and multiple sclerosis primarily affect motor control and balance. Some conditions, including stroke and traumatic brain injury, can simultaneously disrupt both depth perception and coordination through damage to interconnected neural pathways. The distinction determines whether patients should consult an ophthalmologist or neurologist as their primary specialist.
What Are the Key Differences Between Depth Perception and Coordination Impairments?
Depth perception vs coordination impairments: Visual challenges, balance issues, spatial awareness, motor skills comparison
Depth perception and coordination represent distinct neurological functions, though both contribute to spatial awareness and movement precision. Depth perception relies on binocular vision, stereopsis, and the visual cortex to process three-dimensional vision and distance judgment. The retina captures visual information, which the optic nerve transmits to the visual cortex for interpretation of depth cues recognition and spatial relationships.
In contrast, coordination depends on the cerebellum, vestibular system, and motor cortex working together to control movement coordination and postural stability. Proprioception provides sensory feedback about body position, while the inner ear maintains vestibular function and equilibrium problems. According to the American Academy of Ophthalmology (2024), vision disorders causing depth perception issues rarely affect cerebellar function directly.
The central nervous system integrates visual processing with motor planning through the sensorimotor system. When conditions disrupt this cortical integration, patients may experience both visual-spatial deficits and motor skills impairment. The distinction matters because depth perception deficits typically respond to vision therapy and prism glasses, whereas coordination problems require physical therapy and balance training.
Comparison Table: Vision Disorders vs. Neurological Conditions
Vision disorders vs. neurological conditions comparison table: symptoms, causes, diagnosis, treatment.
| Feature | Vision Disorders | Neurological Conditions |
| Primary Impact | Depth perception, stereoscopic vision, distance perception | Motor control, balance control, gait disturbance |
| Common Conditions | Strabismus, amblyopia, cataracts, glaucoma, macular degeneration, convergence insufficiency | Multiple sclerosis, Parkinson’s disease, stroke, cerebellar ataxia, vestibular ataxia |
| Affected Systems | Binocular vision, eye alignment, visual field, peripheral vision | Cerebellum, vestibular system, brainstem, proprioception |
| Assessment Methods | Eye tracking test, stereoacuity test, visual acuity loss measurement | Gait analysis, balance disorder evaluation, proprioceptive input testing |
| Treatment Approaches | Vision therapy, corrective lenses, eye surgery | Physical therapy, occupational therapy, vestibular rehabilitation |
| Primary Specialist | Ophthalmologist, optometrist | Neurologist, physical therapist |
How Do Vision Disorders Impact Depth Perception?
Vision disorders affect depth perception through disruptions in binocular vision dysfunction and stereoscopic depth processing. Strabismus, characterized by eye misalignment, prevents proper eye teaming and convergence ability, reducing three-dimensional vision by approximately 60% according to the American Optometric Association (2023). When the eyes cannot align properly, the brain receives conflicting visual information, impairing depth judgment errors and spatial cognition.
Amblyopia, also known as lazy eye, diminishes visual acuity loss in one eye, forcing reliance on monocular vision and monocular depth perception. Patients lose stereopsis entirely, depending instead on secondary depth cues like object size, shadow patterns, and motion sensitivity. This creates significant distance perception challenges, particularly for tasks requiring fine motor coordination like threading needles or catching objects.
Cataracts and macular degeneration reduce contrast perception and central vision, affecting depth cue processing. According to research published in Ophthalmology (2024), patients with advanced cataracts show 45% reduced accuracy in depth judgment tasks compared to age-matched controls. Glaucoma causes peripheral vision loss and visual field deficits, creating spatial disorientation during navigation and increasing fall risk by 38%.
Diabetic retinopathy damages the retina’s ability to process visual information, affecting both peripheral awareness and central visual processing. Convergence insufficiency prevents proper focusing problems during near tasks, causing double vision (diplopia) and tracking difficulties. Visual processing disorder disrupts how the brain interprets spatial relationships, even when visual acuity remains normal. Conditions like Irlen Syndrome can further complicate visual perception by affecting how the brain processes visual information under certain lighting conditions or patterns.
Which Neurological Conditions Primarily Affect Coordination?
Neurological conditions disrupt coordination through damage to the cerebellum, vestibular system, or sensory integration pathways. Multiple sclerosis causes demyelination of neural pathways, resulting in sensory ataxia, poor coordination, and bilateral coordination deficits. According to the National Multiple Sclerosis Society (2024), approximately 75% of patients experience balance impairment and gross motor function difficulties.
Parkinson’s disease affects motor dexterity and movement precision through dopamine depletion in the motor cortex. Patients exhibit tremors, rigidity, and awkward movements, with fine motor control declining progressively. The condition reduces proprioceptive deficits and kinesthetic feedback, making patients 3 times more likely to experience falls compared to healthy adults.
Stroke can damage the cerebellum or brainstem, causing cerebellar ataxia with unsteady gait and gait abnormalities. Post-stroke patients often struggle with gross motor coordination and hand-eye coordination deficit, requiring extensive occupational therapy. Traumatic brain injury and concussion disrupt vestibular balance and postural balance, with 40% of patients reporting persistent dizziness and equilibrium problems beyond 6 months post-injury.
Developmental coordination disorder (dyspraxia) affects motor planning and visual-motor integration from childhood. Children show clumsiness, stumbling, and tripping during physical activities, with difficulties in both gross motor coordination and fine motor coordination. Vestibular disorders association data (2024) indicates that vestibular impairment causes vertigo symptoms, nystagmus (involuntary eye movements), and severe balance difficulties in 35% of adults over 60.
Can Conditions Affect Both Depth Perception and Coordination Simultaneously?
Several conditions impact both depth perception and coordination through damage to interconnected brain regions. Stroke affecting the visual cortex and cerebellum simultaneously disrupts visual-spatial skills and motor control. According to Stroke (2024), 28% of stroke survivors experience combined deficits requiring both vision therapy and physical therapy.
Traumatic brain injury commonly damages multiple neural pathways, causing vision impairment alongside balance problems. The sensory processing system cannot properly integrate proprioceptive input with visual information processing, resulting in spatial confusion and movement difficulties. Patients report problems with depth perception and coordination together, struggling with tasks like navigating stairs or judging distances while walking.
Multiple sclerosis lesions in the optic nerve cause visual system dysfunction, while cerebellar lesions create vestibular ataxia. This combination produces both depth perception deficits and coordination difficulties, requiring coordinated care from ophthalmologists and neurologists. Concussion frequently causes post-traumatic vision syndrome with convergence problems and oculomotor control issues alongside vestibular function impairment.
Visual processing disorder often coexists with sensory ataxia, particularly in developmental conditions. Children may struggle with depth awareness and body awareness simultaneously, affecting both visual-motor skills and kinesthetic impairment. The perceptual abilities needed for spatial orientation depend on proper cortical integration of sensory feedback from multiple systems.
Use-Case Scenarios: Diagnosis and Treatment Selection
Scenario 1: Pure Depth Perception Deficit
A 45-year-old patient reports difficulty judging distances while driving and frequent near-misses when parking. Vision testing reveals convergence insufficiency with normal neurological function. The optometrist prescribes vision therapy focusing on eye teaming exercises and convergence ability training. After 12 weeks, stereoacuity test results improve by 65%, resolving distance judgment issues.
Scenario 2: Isolated Coordination Problem
A 68-year-old with Parkinson’s disease experiences walking difficulties, unsteady gait, and falls, but maintains normal depth perception. Gait analysis reveals reduced postural stability and motor planning deficits. The physical therapist implements balance training and proprioceptive exercises. After 8 weeks, balance disorder symptoms decrease by 40%, reducing fall risk.
Scenario 3: Combined Deficit Post-Stroke
A 72-year-old stroke survivor exhibits both visual field loss (hemianopia) and cerebellar ataxia. The treatment team includes an ophthalmologist addressing peripheral vision loss through compensatory scanning techniques and a physical therapist working on gait disturbance. Coordinated rehabilitation over 6 months restores functional independence for most daily activities.
Scenario 4: Developmental Coordination Disorder with Visual Component
An 8-year-old child shows poor hand-eye coordination, clumsiness, and difficulty with spatial relationships. Comprehensive evaluation reveals developmental coordination disorder plus mild binocular vision dysfunction. The occupational therapist addresses visual-motor integration while the optometrist treats eye coordination issues. Combined intervention improves fine motor control by 55% over 16 weeks.
How Do Assessment Methods Differ for Depth Perception vs. Coordination Issues?
Evaluating depth perception requires specialized vision testing performed by ophthalmologists or optometrists. The stereoacuity test measures stereoscopic vision using random dot patterns, quantifying depth cue recognition in arc seconds. Eye tracking test technology assesses oculomotor control, convergence ability, and eye teaming during visual tasks. Visual field testing identifies peripheral awareness deficits and central vision problems.
The National Eye Institute (2024) recommends comprehensive eye exams including assessment of binocular depth perception and monocular depth perception separately. Tests measure distance perception accuracy at various ranges, contrast perception under different lighting, and ability to judge distances while moving. Advanced imaging evaluates retina health, optic nerve integrity, and macular degeneration progression.
Coordination assessment uses gait analysis with motion capture technology to quantify balance control and movement precision. Physical therapists measure postural stability using force plate systems, evaluating proprioceptive input and vestibular function. The vestibular disorders association (2024) protocols test for vertigo, nystagmus, and equilibrium problems through specific head movements and balance challenges.
Neurologists conduct neurological function examinations assessing cerebellar function, motor dexterity, and sensory integration. Tests evaluate gross motor function, fine motor coordination, and bilateral coordination through standardized movement tasks. Imaging studies (MRI, CT) identify brainstem lesions, cerebellar ataxia, or other structural causes of motor skills impairment.
What Treatment Approaches Work Best for Each Type of Impairment?
Depth perception issues respond to interventions targeting the visual system. Vision therapy provides structured exercises improving convergence ability, eye alignment, and stereoscopic vision over 8-16 weeks. According to the American Optometric Association (2024), 85% of patients with convergence insufficiency achieve clinically significant improvement through office-based vision therapy combined with home exercises.
Prism glasses correct eye misalignment in strabismus, improving binocular vision and reducing double vision. Surgical correction repositions eye muscles when conservative treatments fail, restoring proper eye teaming in 70-80% of cases. For cataracts and macular degeneration, surgical intervention or low vision rehabilitation helps patients adapt to visual acuity loss and contrast perception changes.
Coordination problems require physical rehabilitation targeting the sensorimotor system. Balance training improves vestibular function and postural stability through progressive exercises challenging equilibrium. Proprioceptive exercises enhance body awareness and spatial orientation through activities emphasizing kinesthetic feedback and sensory processing.
Occupational therapists address fine motor control and visual-motor skills through task-specific training. Gross motor coordination improves through repetitive movement patterns reinforcing neural pathways. Vestibular rehabilitation reduces vertigo symptoms and dizziness in 80% of patients with vestibular impairment within 6-8 weeks. Medication management for conditions like Parkinson’s disease enhances motor cortex function, reducing tremors and improving movement coordination.
Summary Decision Framework: Depth Perception vs. Coordination Focus
Choose depth perception-focused treatment if:
- Primary symptoms include difficulty judging distances, double vision, or focusing problems
- The condition involves strabismus, amblyopia, convergence insufficiency, or visual processing disorder
- Eye tracking test or stereoacuity test reveals binocular vision dysfunction
- Balance and gait remain normal during neurological examination
- An ophthalmologist or optometrist should lead treatment
Choose coordination-focused treatment if:
- Primary symptoms include unsteady gait, falls, clumsiness, or movement precision difficulties
- The condition involves cerebellar ataxia, vestibular ataxia, Parkinson’s disease, or multiple sclerosis
- Gait analysis reveals postural stability or balance control deficits
- Vision testing shows normal depth perception and eye alignment
- A neurologist, physical therapist, or occupational therapist should lead treatment
Choose combined treatment approach if:
- Condition involves stroke, traumatic brain injury, or concussion affecting multiple brain regions
- Both vision testing and neurological examination reveal abnormalities
- Patient experiences spatial disorientation, poor hand-eye coordination, and balance impairment
- Symptoms suggest disrupted cortical integration and sensory processing
- Coordinated care from ophthalmology, neurology, and rehabilitation specialists is necessary
Understanding whether a condition primarily affects depth perception or coordination determines the appropriate specialist, assessment methods, and treatment approach. While vision disorders typically impair spatial perception and three-dimensional vision, neurological conditions predominantly disrupt motor control and vestibular balance. Some conditions require addressing both visual system dysfunction and cerebellar function simultaneously for optimal outcomes. Accurate diagnosis through comprehensive testing enables targeted interventions that restore functional abilities and reduce fall risk.